
Febre Q com Envolvimento Isolado da Medula Óssea
DOI:
https://doi.org/10.24950/rspmi.2616Palavras-chave:
Coxiella burnetii, Febre Q/complicações, Medula ÓsseaResumo
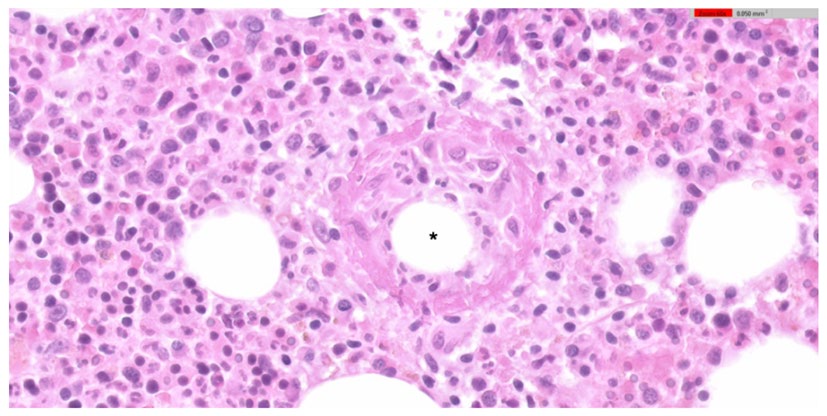
Homem de 71 anos recorreu ao serviço de urgência com 3 semanas de febre, astenia e suores nocturnos. Os resultados laboratoriais iniciais mostraram anemia ligeira, trombocitopenia e elevação da proteína C reativa, com enzimas hepáticas normais. O restante estudo inicial foi inconclusivo. Devido às anomalias hematológicas, foi realizada biópsia da medula óssea que revelou múltiplos granulomas epitelioides em anel, que consistiam num vacúolo lipídico central rodeado por células epitelioides e alguns neutrófilos. Estes achados, embora não patognomónicos, favoreceram o diagnóstico de febre Q com envolvimento isolado da medula óssea. O diagnóstico foi posteriormente confirmado com seroconversão e exclusão de outras causas para este achado histopatológico. O paciente foi tratado com doxiciclina durante catorze dias, com boa resposta e sem evidência da doença ao fim de seis meses.
Downloads
Referências
1. Eldin C, Melenotte C, Mediannikov O, Ghigo E, Million M, Edouard S, Mege JL, et al. From Q Fever to Coxiella burnetii Infection: a Paradigm Change. Clin Microbiol Rev. 2017;30:115-190. doi:10.1128/CMR.00045-16.
2. Maurin M, Raoult D. Q fever. Clin Microbiol Rev. 1999;12:518-553.
3. Anderson A, Bijlmer H, Fournier PE, Graves S, Hartzell J, Kersh GJ, et al. Diagnosis and management of Q fever - United States, 2013: recommendations from CDC and the Q Fever Working Group. MMWR Recomm Rep. 2013;62:1-30.
4. Alves J, Almeida F, Duro R, Ferraz R, Silva S, Sobrinho-Simoes J, et al. Presentation and diagnosis of acute Q fever in Portugal - A case series. IDCases. 2017;7:34-37. doi:10.1016/j.idcr.2016.11.002.
5. Palmela C, Badura R, Valadas E. Acute Q fever in Portugal. Epidemiological and clinical features of 32 hospitalized patients. Germs. 2012;2:43-59. doi:10.11599/germs.2012.1013.
6. Kreisel F. Doughnut ring-shaped epithelioid granulomas in the bone marrow of a patient with Q Fever. Int J Surg Pathol. 2007;15:172-3. doi:10.1177/1066896906299074.
7. Melenotte C, Protopopescu C, Million M, Edouard S, Carrieri MP, Eldin C, et al. Clinical Features and Complications of Coxiella burnetii Infections From the French National Reference Center for Q Fever. JAMA Netw Open. 2018;1:e181580. doi:10.1001/jamanetworkopen.2018.1580.
8. Fournier PE, Marrie TJ, Raoult D. Diagnosis of Q fever. J Clin Microbiol. 1998;36:1823-34. doi:10.1128/JCM.36.7.1823-1834.1998.
9. Lamps LW. Hepatic granulomas, with an emphasis on infectious causes. Adv Anat Pathol. 2008;15:309-18. doi:10.1097/PAP.0b013e31818a6477.
10. Raya Sanchez JM, Arguelles HA, Brito Barroso ML, Nieto LH. Bone marrow fibrin-ring (doughnut) granulomas and peripheral T-cell lymphoma: an exceptional association. Haematologica. 2001;86:112.
11. Bernstein M, Edmondson HA, Barbour BH. The liver lesion in Q fever. Clinical and pathologic features. Arch Intern Med. 1965;116:491-8.
12. Glazer E, Ejaz A, Coley CJ, Bednarek K, Theise ND. Fibrin ring granuloma in chronic hepatitis C: virus-related vasculitis and/or immune complex disease? Semin Liver Dis. 2007;27:227-30. doi:10.1055/s-2007-979473.
13. Wegdam-Blans MC, Kampschreur LM, Delsing CE, Bleeker-Rovers CP, Sprong T, van Kasteren ME, et al. Chronic Q fever: review of the literature and a proposal of new diagnostic criteria. J Infect. 2012;64:247-259. doi: 10.1016/j.jinf.2011.12.014.
14. Limonard GJ, Peters JB, Besselink R, Groot CA, Dekhuijzen PN, Vercoulen JH, et al. Persistence of impaired health status of Q fever patients 4 years after the first Dutch outbreak. Epidemiol Infect. 2016;144:1142-7. doi:10.1017/S0950268815002216.
15. van Roeden SE, van Houwelingen F, Donkers CM, Hogewoning SJ, de Lange MMA, van der Hoek W, et al. Exposure to Coxiella burnetii and risk of non-Hodgkin lymphoma: a retrospective population-based analysis in the Netherlands. Lancet Haematol. 2018;5:e211-e219. doi:10.1016/S2352-3026(18)30038-3.
Downloads
Publicado
Como Citar
Edição
Secção
Categorias
Licença
Direitos de Autor (c) 2025 Medicina Interna

Este trabalho encontra-se publicado com a Licença Internacional Creative Commons Atribuição 4.0.





